Overview
This project was part of the EKA IxD.ma "Design for Social Innovation" course (2020), run in partnership with the North Estonia Medical Centre (PERH) — one of the country's top healthcare providers and its highest-competence regional hospital. Twelve interaction designers were given four challenges sourced from PERH personnel, of which each team chose one. We chose Challenge 3: Reaching the Life Savers.
PERH employs over 5,000 people. Effective internal communication is critical — especially during COVID, when rules for in-house conduct and navigation had to be followed precisely. The starting question we were handed: how do we reach, promptly, those employees who don't use computers on a daily basis?
The course ran over 7 weeks: research & framing (weeks 1–3), concept development (week 4), validation through user testing (weeks 5–6), and communication/documentation (week 7).
Key Outcomes
Problem statement
How do we reach promptly those employees who don't use computers on a daily basis?
Research & Discovery
We scoped the challenge down to critical messages that need to reach everyone quickly — the information people need to act correctly and safely at work. PERH is a large, deeply nested organisation: its official structure has 8 clinics, broken down into ~35 centres and dozens of departments and units below them. Critical messages originate from board meetings or the infection-control department, and are owned by the Internal Communications team, who distribute them digitally and rely on department leads to pass them down.
The existing channel mix: intranet, an email list, a weekly Monday newsletter, a leaders' meeting, departmental message boards and posters, a voluntary weekly all-staff info meeting, and (rarely) SMS to department leads. The crucial at-risk group was nurses and caregivers, who are often too busy to access a computer and so might miss critical information — and crucially, no one was collecting feedback on whether messages actually landed or were acted on.
We worked with Hede Kerstin Luik, Andra Prems, and Stina Eilsen from the Communications Department, and planned to deliver an audit of the current flow (AS-IS) and a prototype of an improved flow (TO-BE).
Interviews
We conducted 8 interviews: 3 heads of service, 2 service workers, 1 director of nursing, 1 head of nursing (department level), and 1 caregiver. Interviews were run in pairs — one person interviewing, one taking notes — and recorded for transcription. I took part in the interviews directly.

Key finding — computers aren't necessary. As one interviewee put it:
"Head of Nursing calls and brings me printed-out info about new rules."
Messages already get through offline, via:
- Regular daily meetings
- Face-to-face communication with a direct manager
- Pen-and-paper notes and printouts
In short — "Good job, PERH!" The original problem already had working informal solutions in place. This was the turning point that made us rethink the entire direction.
Mapping the Information Flow
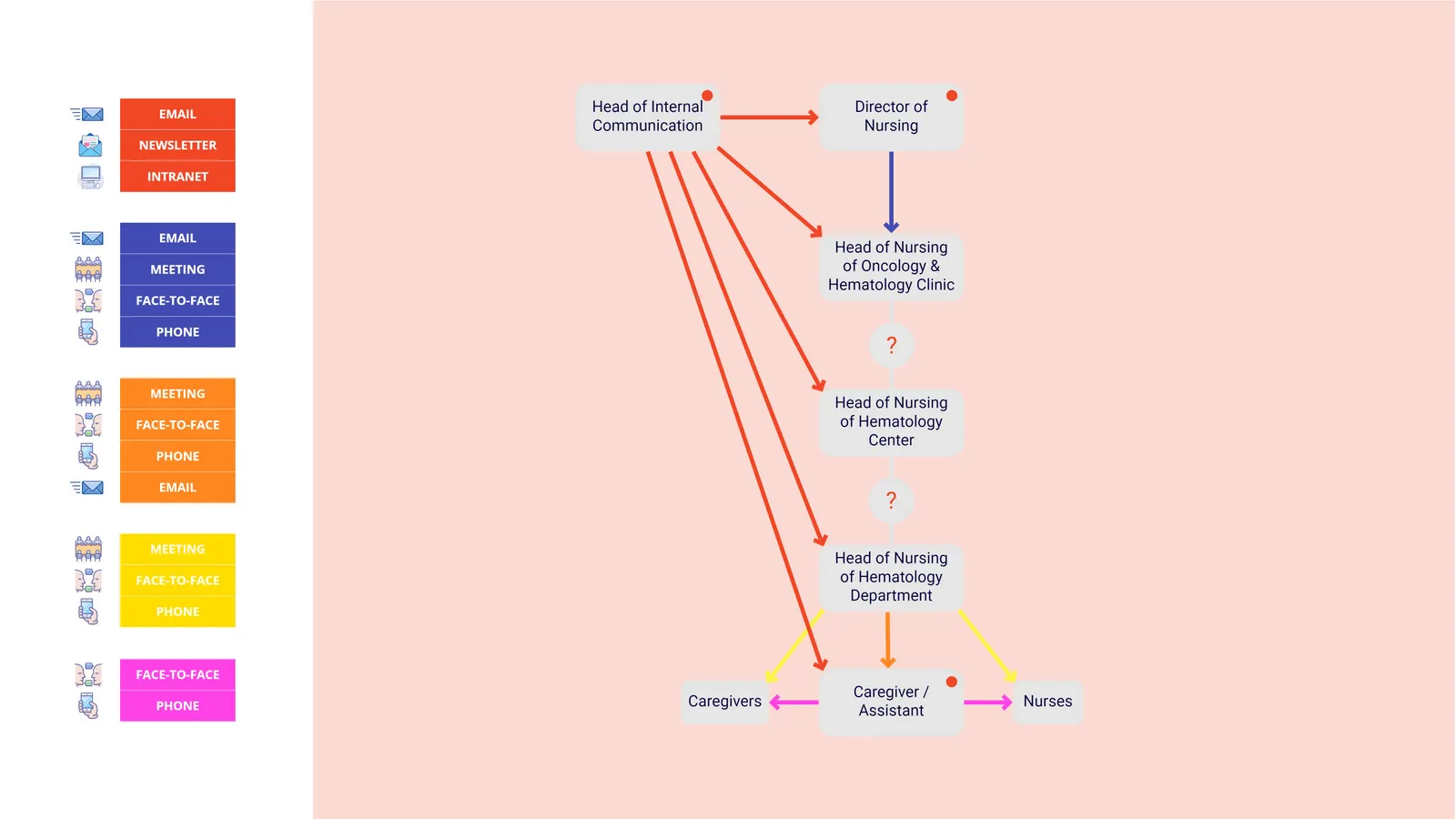
To make the existing flow legible, we mapped it across the org chart — splitting the hospital into its administrative side (Board → Chairman / Board Member → Head of Internal Communication, Director of Administrative Services, Head of Infection Control → Manager of Administrative Services → Cloakroom Attendant, Hostess) and its medical side (Chief Physician → Director of Treatment, Director of Nursing → clinic / centre / department heads of nursing → Nurses & Caregivers).
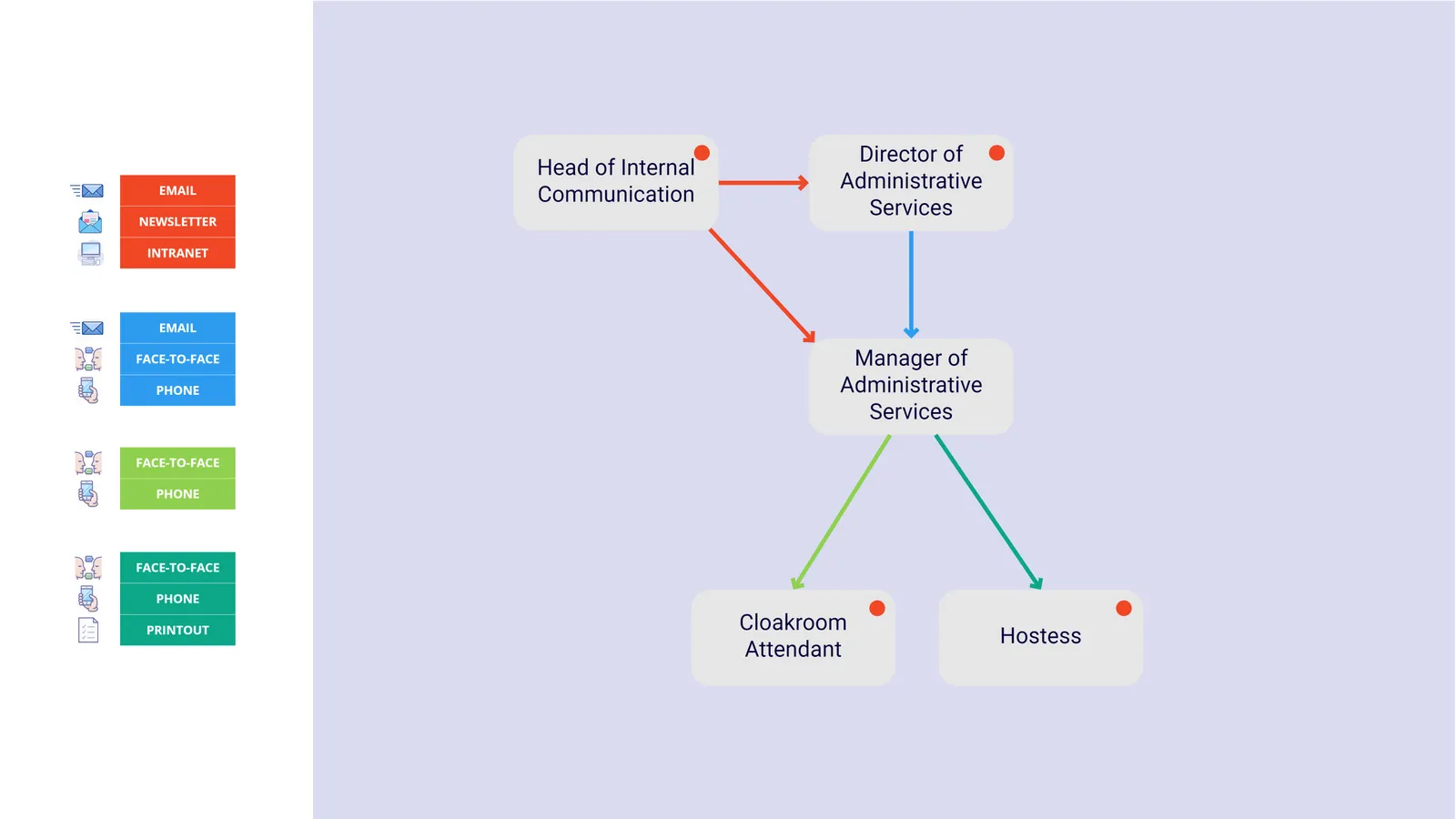
Two things stood out in the maps:
Channel richness degrades down the chain. Senior roles communicate via email, newsletter, and intranet; by the time a message reaches the people at the bottom, it's arriving mostly through face-to-face, phone, and printouts.
The bottom of the chain is unmapped. Between the lower nursing levels and actual nurses/caregivers, we repeatedly hit handoffs we couldn't confirm (marked "?" on the maps). The closer we got to the frontline, the less anyone could say with certainty how a message actually arrives.
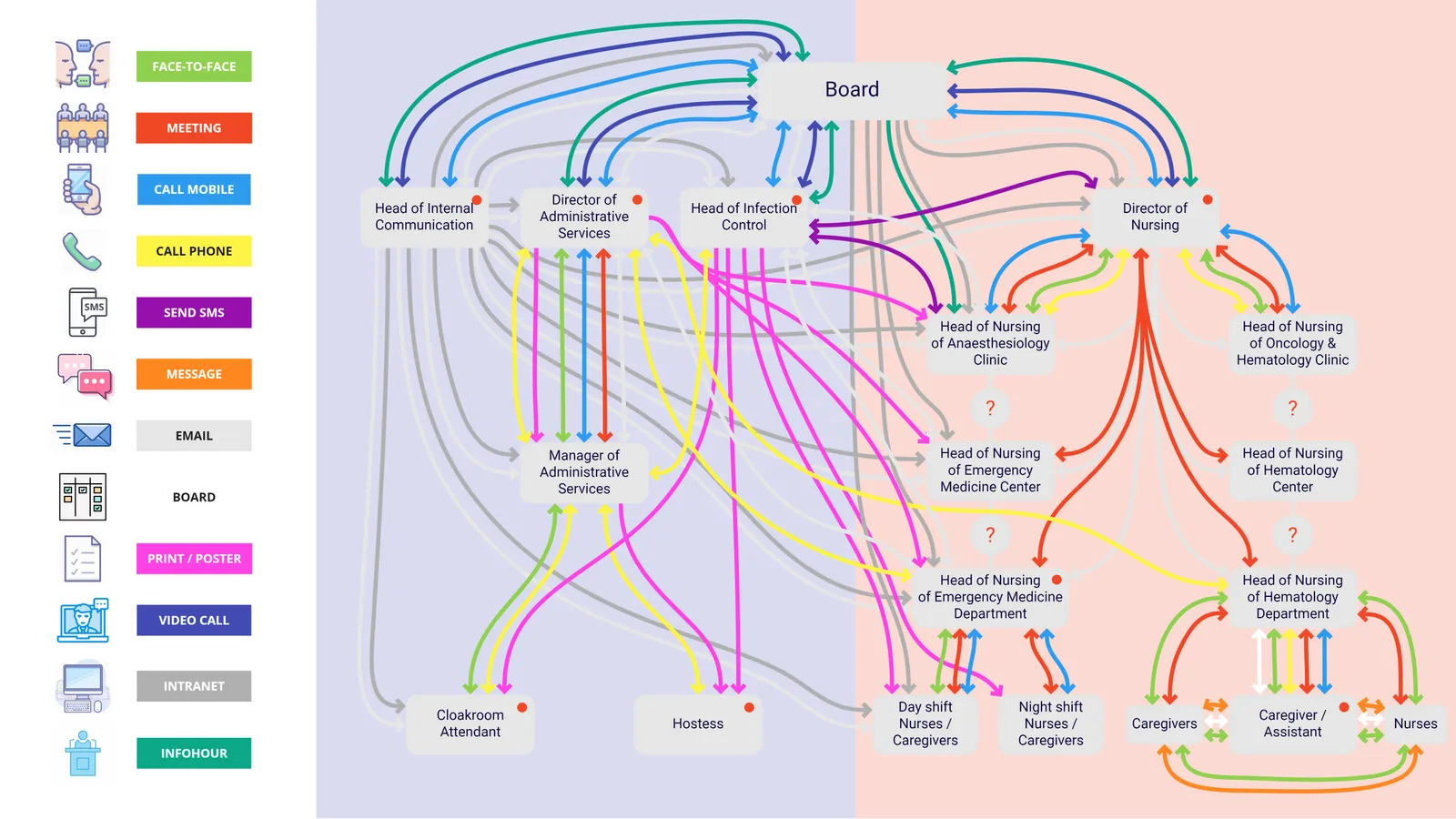
Interview coverage spanned both sides of the org chart — Head of Internal Communication, Director of Administrative Services, Head of Infection Control, Cloakroom Attendant, and Hostess on the administrative side; Director of Nursing, a department-level Head of Nursing, nurses/caregivers, and a caregiver/assistant on the medical side.
Reframing the Problem
Because the original communication problem was already largely solved through informal, offline channels, we shifted focus to employee engagement and company culture — "So what happens between the people?"
Exploration
To dig into the new direction, we:
- Gathered information from other EKA teams
- Went through old interviews with fresh eyes
- Conducted new interviews
- Read through PERH's public documents
This led us to a line from PERH's own strategy that matched our direction:
"Focus on developing a hospital environment and working culture that is based on patient needs and supports employee engagement."
The Missing Element
Looking specifically at nurses & caregivers at PERH, three findings stood out:
1. Nurses & caregivers show great initiative in creating a pleasant working atmosphere
"But of course! For example, I have a birthday tomorrow, so we will have a party here!"
"Our department has very strong teamwork. It means that people trust each other, and that is most important. We — doctors, nurses and caregivers — talk to each other as family members."
2. Nurses' & caregivers' knowledge doesn't reach leadership for decision-making
"I asked for a few small tables instead of one big one, so people can sit in groups, but got a big table. It's also bolted to the ground."
"If it's a patient problem, it will be solved. But if I have something that needs to be done, it is not done."
3. Leadership lacks an overview of employee engagement
"It would be interesting to know where caregivers get their info."
"Would be interesting to know what information space they live in."
The Representation Gap
Nurses and caregivers were strikingly underrepresented in PERH's public communications:
Nurses and caregivers make up roughly 54% of PERH's workforce, yet account for only about ~10% of representation in public communications — a clear mismatch between who does the work and who gets seen.
Design challenge
How might we shine a light on nurses and caregivers to build a better PERH together?
Design Guidelines
Leverage initiative
Bring nurses' & caregivers' initiative to leadership
Use existing tools
Build on tools already in use, like pen & paper
Use time efficiently
Make it asynchronous — no time taken from patient care
Solution: Cultur-O-meter
A physical board concept, co-developed with PERH + EKA, designed to sit in shared staff spaces.
The Board
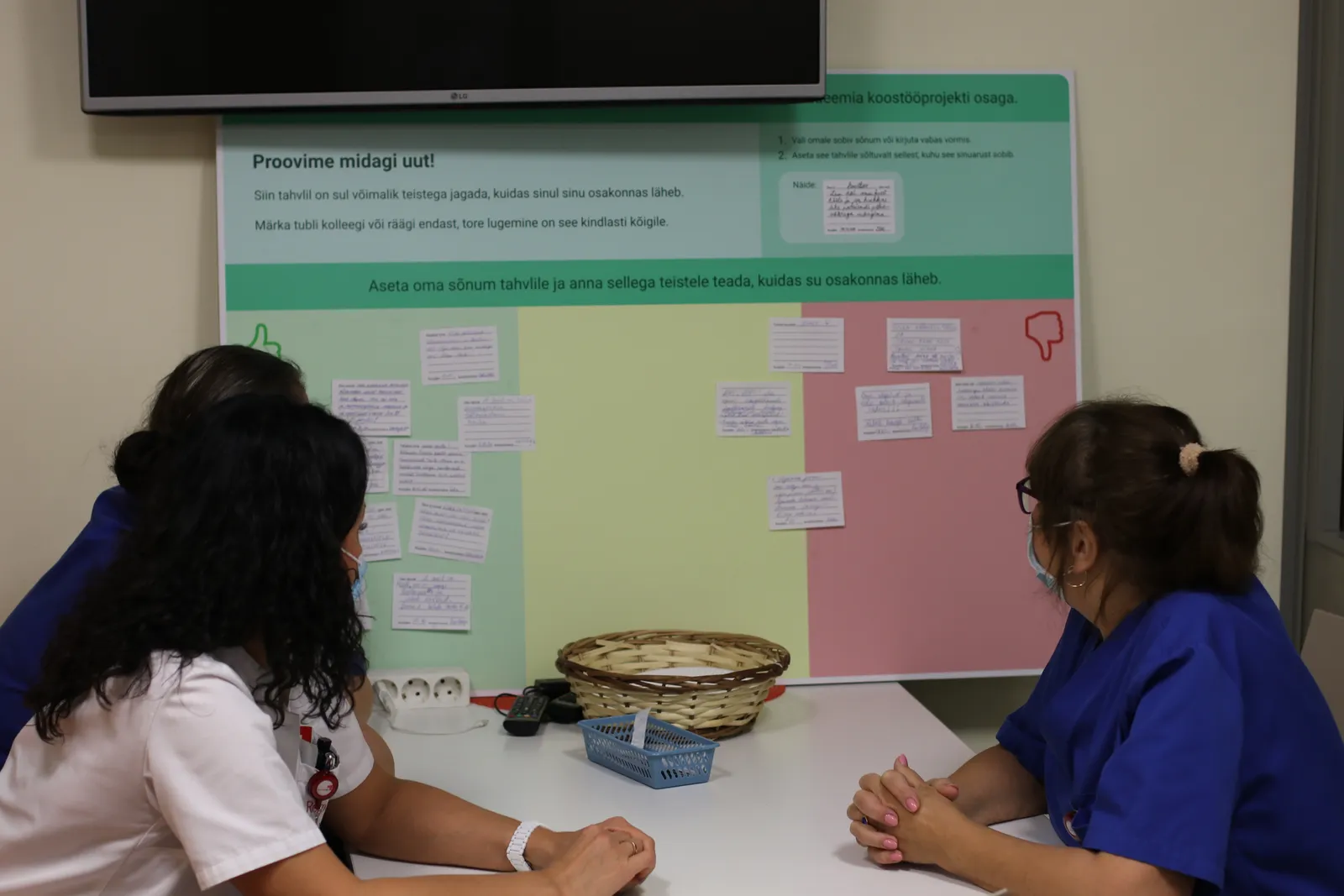
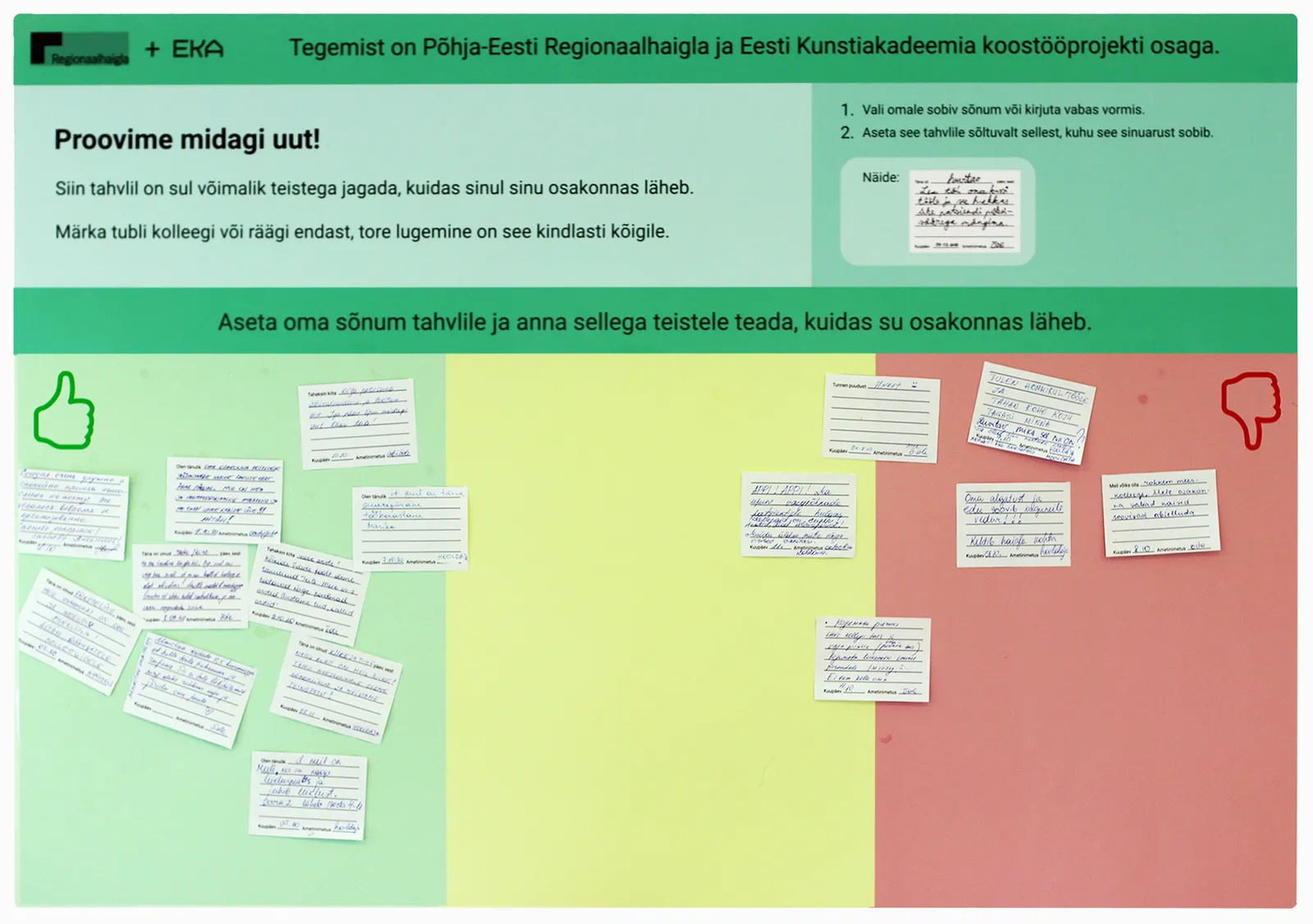
A large-format (A0) printed board, co-branded Regionaalhaigla + EKA, headed "Proovime midagi uut!" ("Let's try something new!"). It invites staff to share how things are going in their department, notice a good colleague, or speak about themselves. Simple two-step instructions plus an example show how to fill a card and place it on the board.
Three colour zones — green (positive / thumbs-up), yellow (in-between), and red (negative / thumbs-down) — encourage positivity while leaving room for more difficult topics.
The Cards
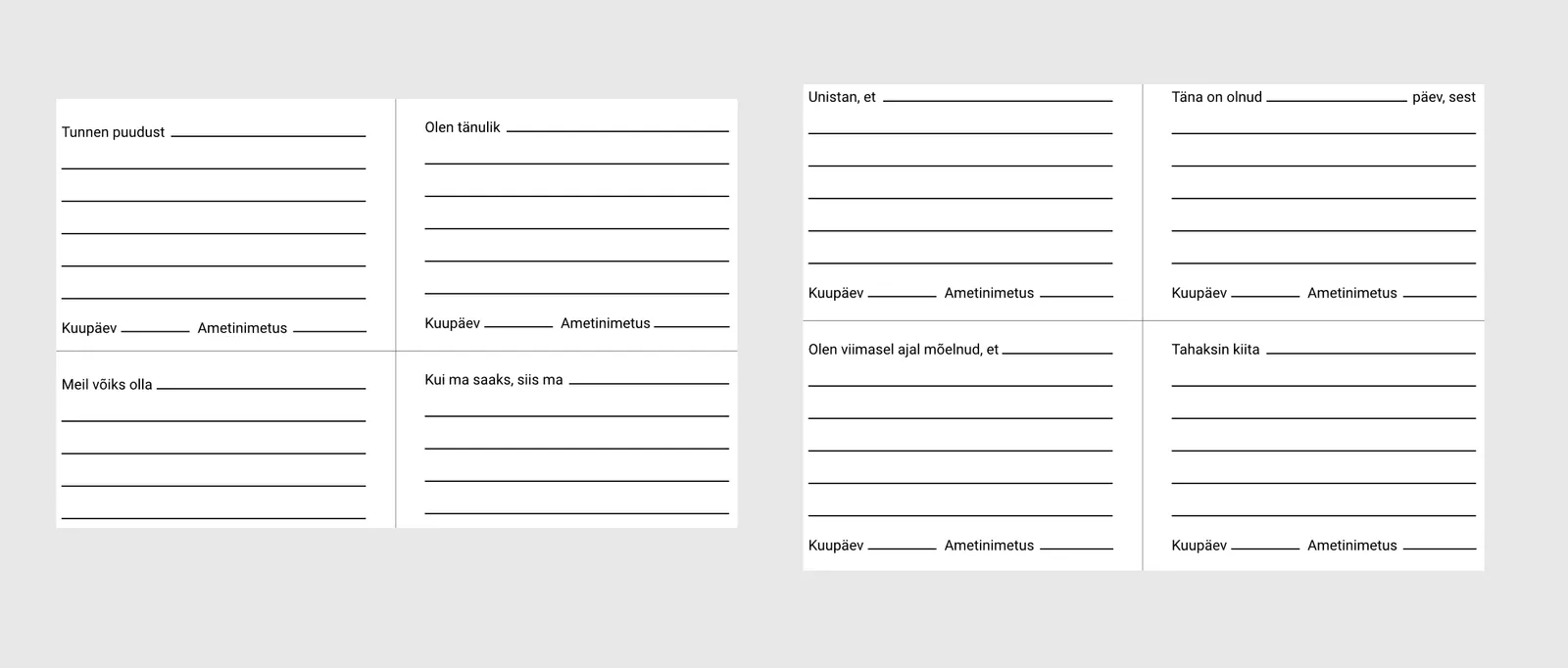
A4 cards (printed two-up per A7 sheet) with sentence starters, designed to spark reflection and lower the barrier to writing something down. Each card has space for the message plus fields for date (Kuupäev) and job title (Ametinimetus). The 8 printed prompts:
Unistan, et… — "I dream that…"
Olen viimasel ajal mõelnud, et… — "Lately I've been thinking that…"
Tunnen puudust… — "I miss…"
Meil võiks olla… — "We could have…"
Täna on olnud … päev, sest… — "Today has been a … day, because…"
Tahaksin kiita… — "I'd like to praise…"
Olen tänulik… — "I'm grateful…"
Kui ma saaks, siis ma… — "If I could, I would…"
Plus blank cards (same date/title fields, no prompt) for fully free-form messages.
Value for Both Sides
For nurses & caregivers
- Gratitude creates more gratitude
- Undercover role modeling — seeing peers express praise/reflection encourages others to do the same
For managers
- Acts as a backlog of problems/ideas to bring to higher management
- A way to monitor team health over time
- Material for the communications team to spotlight nurses and caregivers
Constraints
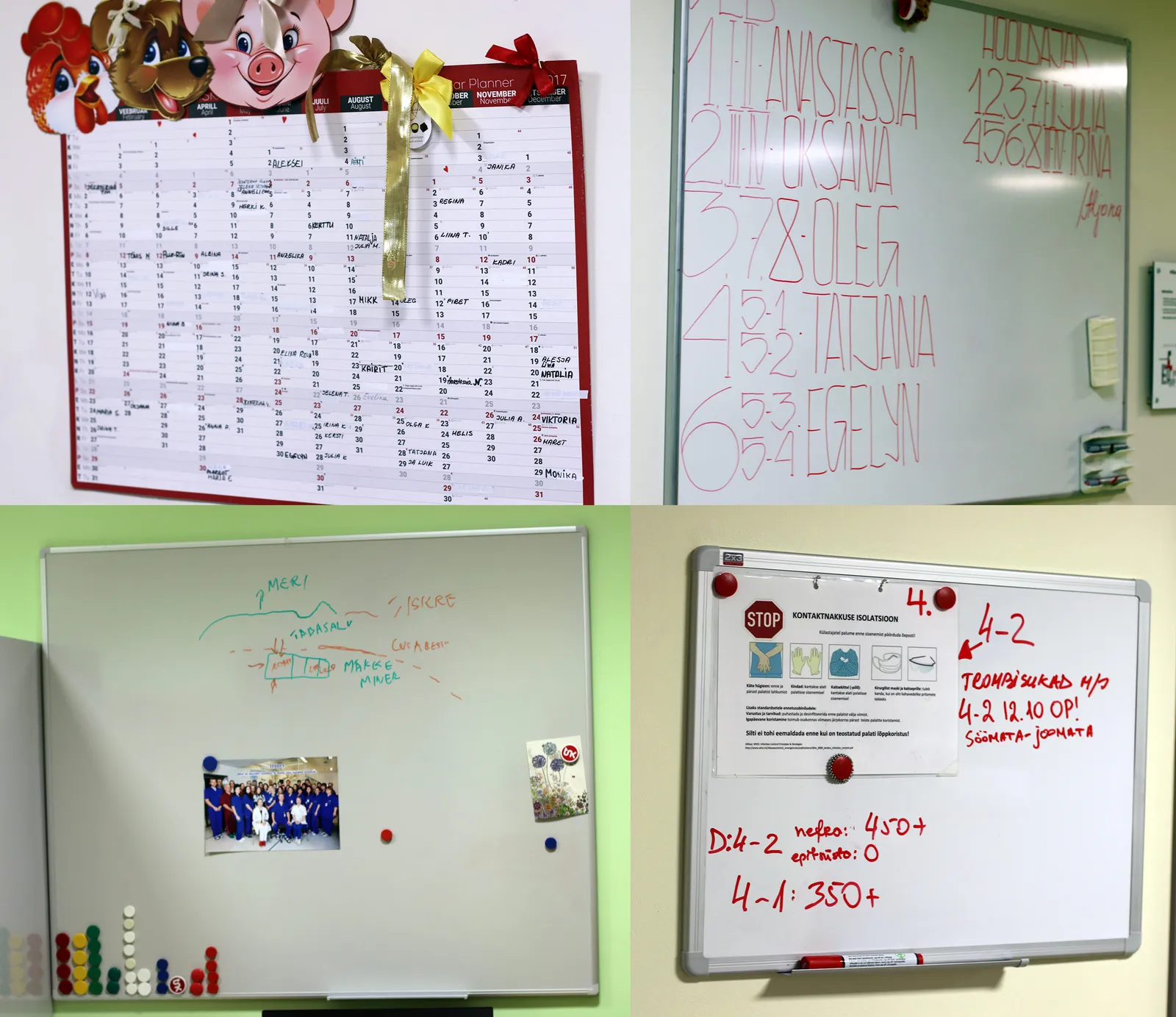
- The solution had to fit into existing physical habits — many departments already used whiteboards, bulletin boards, and wall calendars for informal tracking, so the board needed to slot into that same space and behaviour.
- It needed to work asynchronously, without taking time away from patient care.
- Designed to double as a break-time activity, fitting into staff's limited downtime.
- The 7-week project timeline meant the concept had to be testable quickly, not polished to perfection.
Pilot Testing
We ran a short pilot across 3 departments over 5 days (Wednesday to Monday):
Feedback
- Risk that the board becomes "wallpaper" over time if not refreshed
- Patient praise notes were shared in team meetings
- Managers were already aware of most of the flagged problems — validating that the board surfaces real issues, not noise
Second Iteration
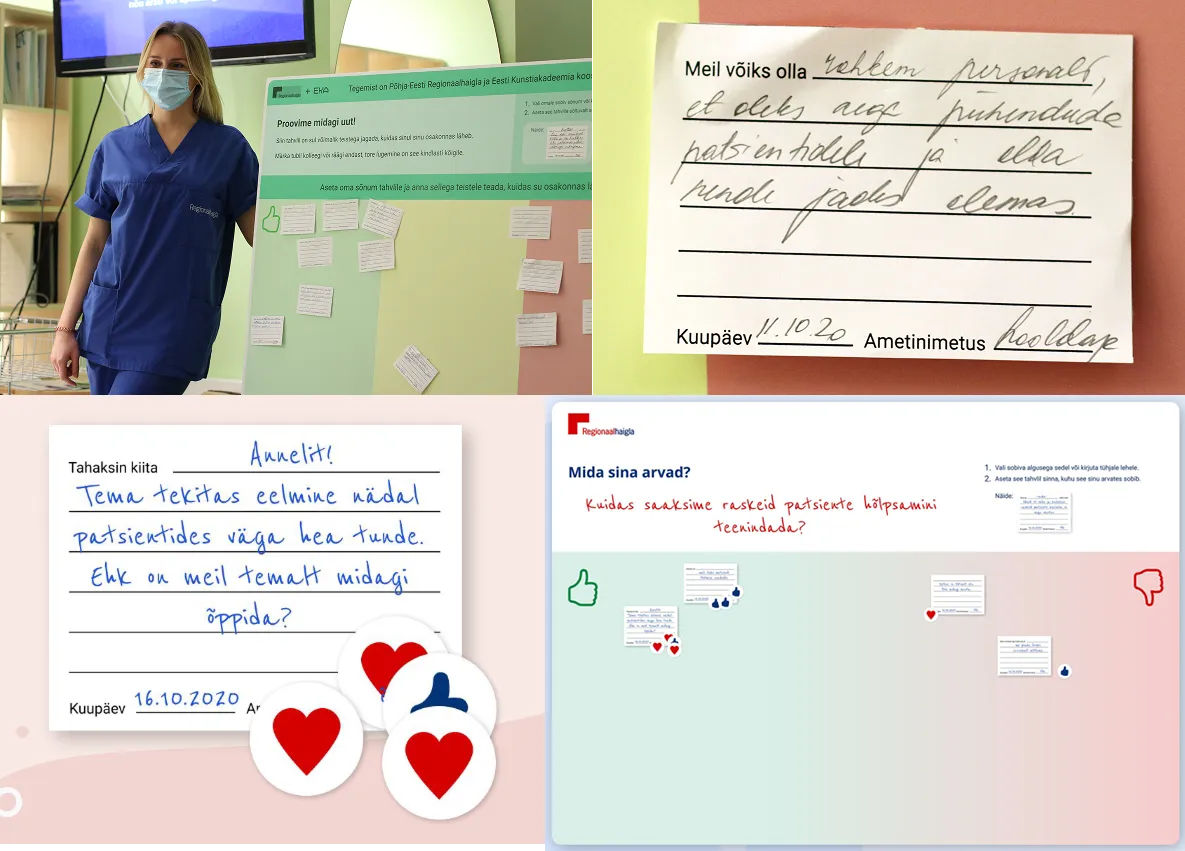
We tested a more focused version with a specific prompt question: "Kuidas saaksime raskeid patsiente hõlpsamini teenindada?" ("How could we make it easier to care for difficult patients?")
Colleagues responded directly to each other's notes using reaction stickers (thumbs-up, hearts) — a note praising a colleague named Anneli for boosting patient mood received multiple heart reactions, and a "wish list" note about patient-lifting equipment got thumbs-up support.
The second iteration showed that focused prompts and peer reactions generated richer, more actionable feedback than the open-ended first version.
Learnings
Clearer prompts guide better output. Open-ended boards risk becoming "wallpaper" — specific questions generated more focused, actionable responses.
Employee praise needs active encouragement. Positive feedback doesn't flow naturally in a high-stress environment — it needs to be prompted and modeled.
Visible follow-through matters most. Staff need to see that their input leads to actual change, otherwise participation drops.
Nothing beats meeting people where they already are. The biggest lever was building on tools people already use and are comfortable with — pen, paper, a wall — rather than introducing anything new to learn. Familiarity lowered the barrier to participation more than any feature could.
Next Steps for PERH
- Use the "early adopter" group/department for a longer pilot run
- Define themes and topics to test the boards with
- Determine who is responsible for maintaining the board
"If we had 7 weeks to solve a problem, we would spend 6 weeks thinking about the problem and 1 week solving it."
— (slightly edited) Albert Einstein